PLANTAR FASCIITIS
Heel pain • First-step pain • Modern treatment options
Fast, patient-centered care for chronic heel pain — from proven conservative options to advanced minimally invasive Plantar Fasciitis Embolization (PFE) for select patients whose symptoms persist.
- Most people improve with a structured conservative program.
- Open surgery exists but is typically reserved for refractory cases after months of treatment.
- PFE is emerging—early reports and trials are building the evidence base.

Where it hurts: most often the inner underside of the heel where the plantar fascia attaches.
New Patient? Start Here
Get your visit moving quickly: complete paperwork, confirm insurance, and request an appointment.
About plantar fasciitis
What is plantar fasciitis?
The plantar fascia is a strong band of tissue under the foot that supports the arch. With overload and repetitive strain, the heel attachment can become painful—often worst with the first steps in the morning.
Common condition
- Typical location: medial plantar heel pain.
- Typical pattern: “first-step pain” after rest.
- Key principle: reduce load + restore flexibility + strengthen support.
Affected area
Visual: where plantar fasciitis lives
Click-through images are kept simple and fast-loading for a marketing page. If you want a deeper clinical gallery (ultrasound/MRI/angiography), we can add it below the PFE section.

Pain location

Anatomy
Plantar fascia under the foot.
Symptoms
How it feels
Symptoms often develop gradually and may worsen with prolonged standing, new exercise, or changes in footwear.
- Sharp or aching pain under the heel (often inside/medial side).
- Worse with first steps in the morning or after sitting.
- Can flare after long periods on your feet.
- May coexist with calf tightness/Achilles tightness.

First-line care
Conservative treatments

Stretching & mobility
Plantar fascia stretching + calf/Achilles stretching are cornerstone therapies.
Footwear & support
Supportive shoes, heel cups, and orthoses can reduce pain and improve function.

Advanced conservative options
For recalcitrant cases: PT, injections, and extracorporeal shockwave therapy (ESWT).
A simple starter plan
6–8 week program
- Daily plantar fascia–focused stretching + calf stretching
- Supportive footwear (including at home), consider OTC orthotic + heel cup
- Reduce impact temporarily; gradual return as pain improves
- Ice massage after activity; NSAIDs only if appropriate
- Reassess if symptoms persist despite good adherence
When conservative care fails
Open surgical options
Surgery is typically considered after prolonged, structured conservative therapy. Options may include partial plantar fasciotomy or gastrocnemius recession, depending on biomechanics and exam findings.
- Open/partial plantar fasciotomy (release): reduces tension but carries risks (scar pain, nerve irritation, biomechanical changes).
- Gastrocnemius recession: addresses calf tightness driving heel overload; outcomes can be favorable in select patients.
- Important: accurate diagnosis matters—other problems can mimic plantar fasciitis.
Your advantage
Modern alternatives before surgery
Signature minimally invasive option
Plantar Fasciitis Embolization (PFE)
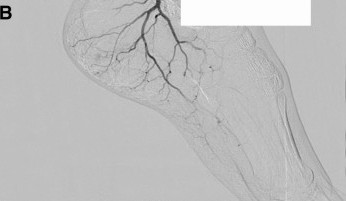
PFE (also described as transarterial embolization/microembolization for plantar fasciitis) is an image-guided outpatient procedure intended to reduce abnormal “pain blood vessels” (neovessels) associated with chronic plantar fascia irritation.
Why patients love it
Simple. Targeted. No open incision.
- Minimally invasive: tiny access site (no open heel incision).
- Fast: published case reports describe very short procedure times.
- Outpatient: typically same-day with rapid return to daily activity (provider-specific instructions apply).
Before
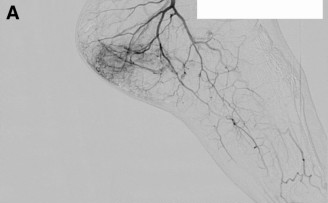
After